Complex regional pain
syndrome (CRPS)
Many chronic conditions are challenging to manage. Here we focus on eight key pain conditions with a high unmet need among patients and/or healthcare professionals.
Our aim here is to provide the pain community with in-depth information about these conditions; from disease understanding to management approaches.
Complex regional pain syndrome (CRPS) is a chronic pain condition characterised by continuing (spontaneous and/or evoked) regional pain, usually beginning in a distal extremity, that is disproportionate in time or degree to the usual course of pain after trauma or other lesion.1,2 It is distinguished from other chronic pain conditions by the presence of signs indicating prominent autonomic and inflammatory features.2 There are two types of CRPS: type 1 presents with no obvious nerve lesion following an injury (reflex sympathetic dystrophy) and type 2 describes CRPS where there is a definite nerve injury (causalgia).3,4
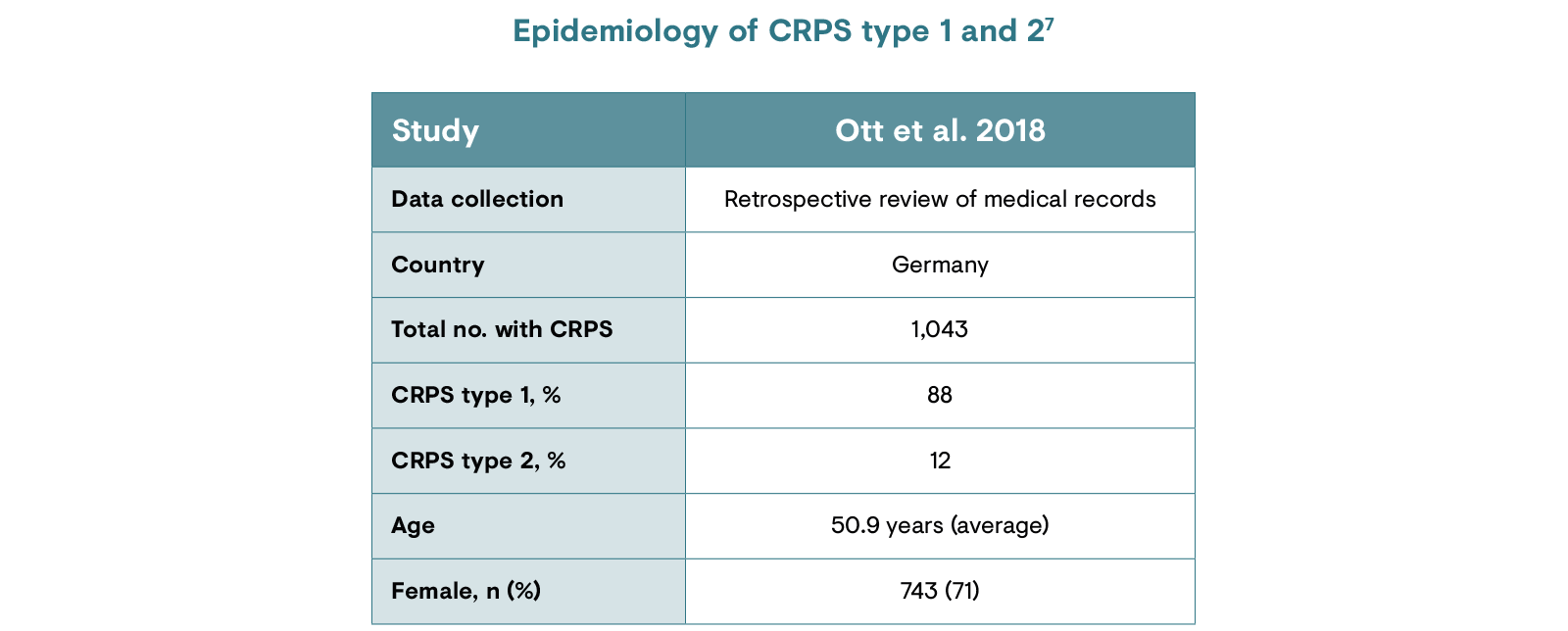
The precise prevalence of CRPS is difficult to determine; recent results from major epidemiological studies suggest that the incidence is between 5.5 and 26.2 cases per 100,000 people per year.6 Variations in these figures may occur as a result of differential diagnostic criteria and difficulties in diagnosing this complex condition. CRPS appears to occur more frequently in women aged between 40 and 60 years6 and the majority of patients present with CRPS type 1.7 Data on the most common localisation of pain are scarce.
CRPS: complex regional pain syndrome.
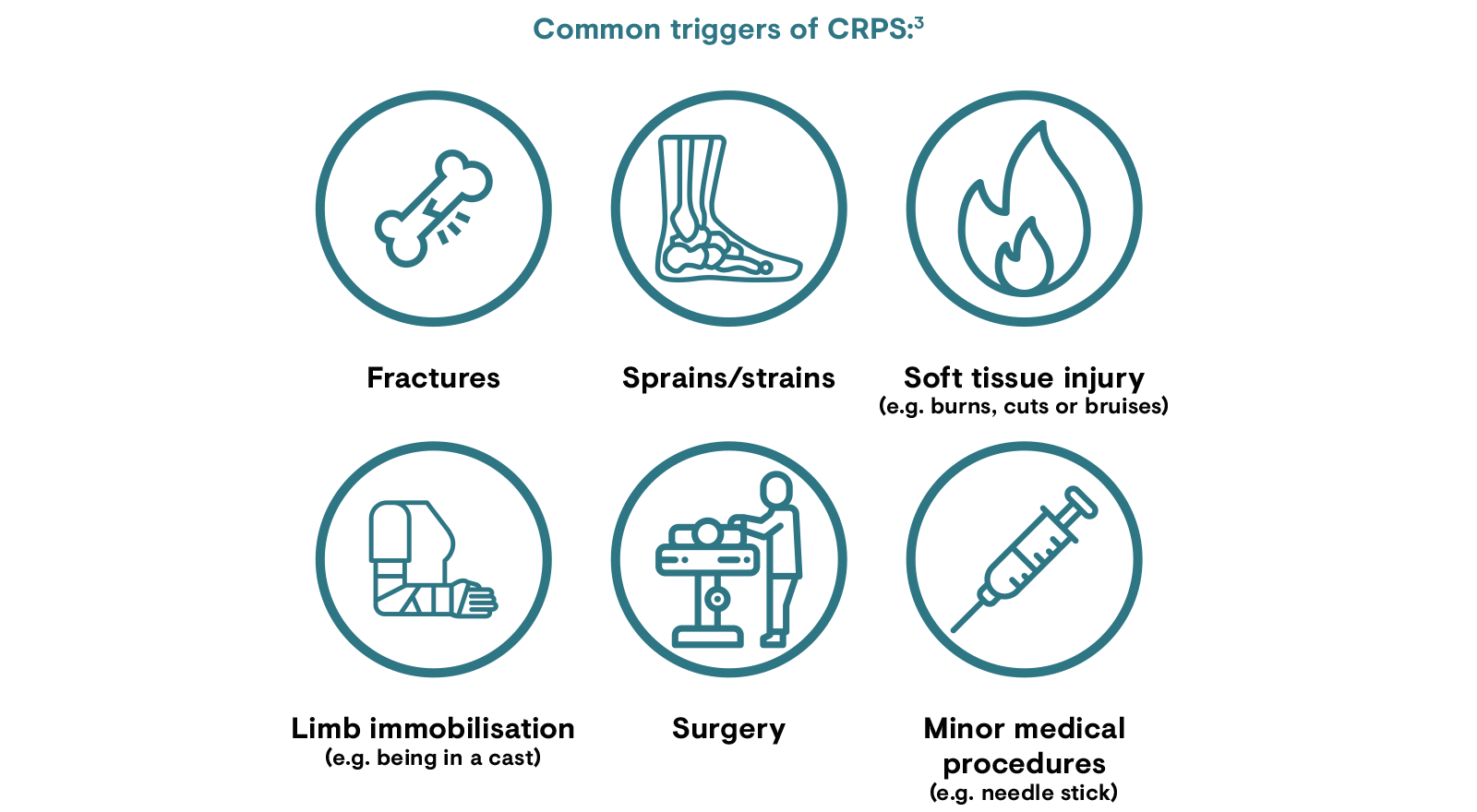
CRPS typically occurs following a trauma or injury to a limb, including fractures, sprains/strains, operations and burns, with a particular risk associated with immobilisation and ankle dislocation or intra-articular fracture.8 The risk of CRPS is higher for patients exhibiting complicated fractures, rheumatological disease or those who present with intense pain 1 week after trauma, compared with those without these characteristics.6 CRPS occurs more in women, though this higher prevalence could be attributed to women’s more frequent radial fracture rate when compared with men.5

While it is unclear why a similar trauma leads to the development of CRPS in some individuals and not others, it is established that the majority of CRPS cases are associated with trauma or injury.3 While the exact mechanism is unknown, the response to injury in patients with CRPS appears to be exaggerated.3,12 CRPS may bring about an abnormal response that magnifies the effects of the initial injury.3
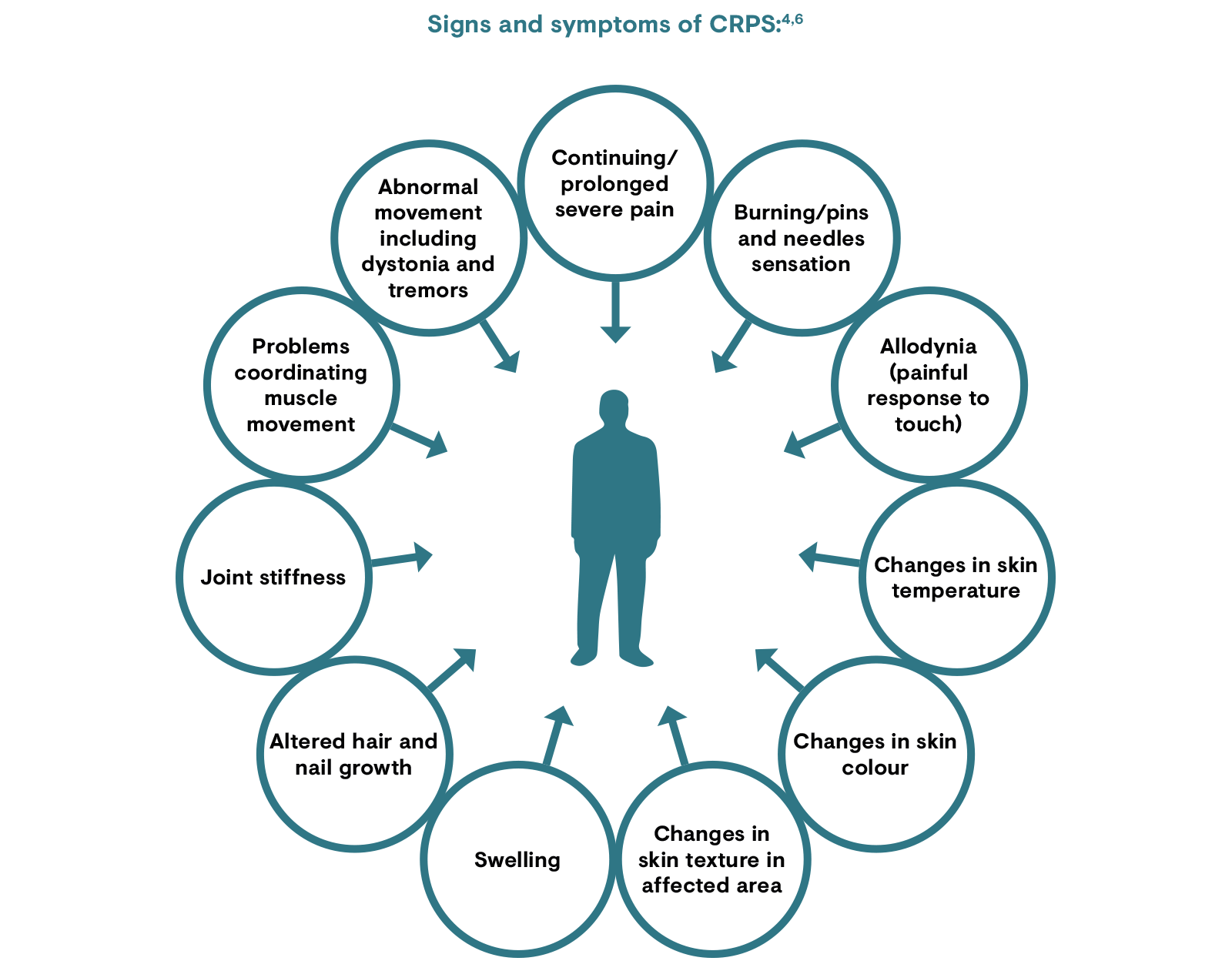
The key symptom of CRPS is continuing pain, which is disproportionate to any inciting event.2 The pain has been described as ‘burning, stabbing, tingling numbness’, ‘pins and needles’, ‘electric shock’ or as if somebody were squeezing the limb in question.3,4 The pain can spread to the entire limb and may even affect the opposite extremity.4 Alongside pain, other symptoms include changes in skin temperature, colour or swelling. Other features include changes in skin texture in the affected area, abnormal sweating, changes in nail and hair growth, stiffness in affected joints, problems coordinating muscle movement and abnormal movement in that area.4
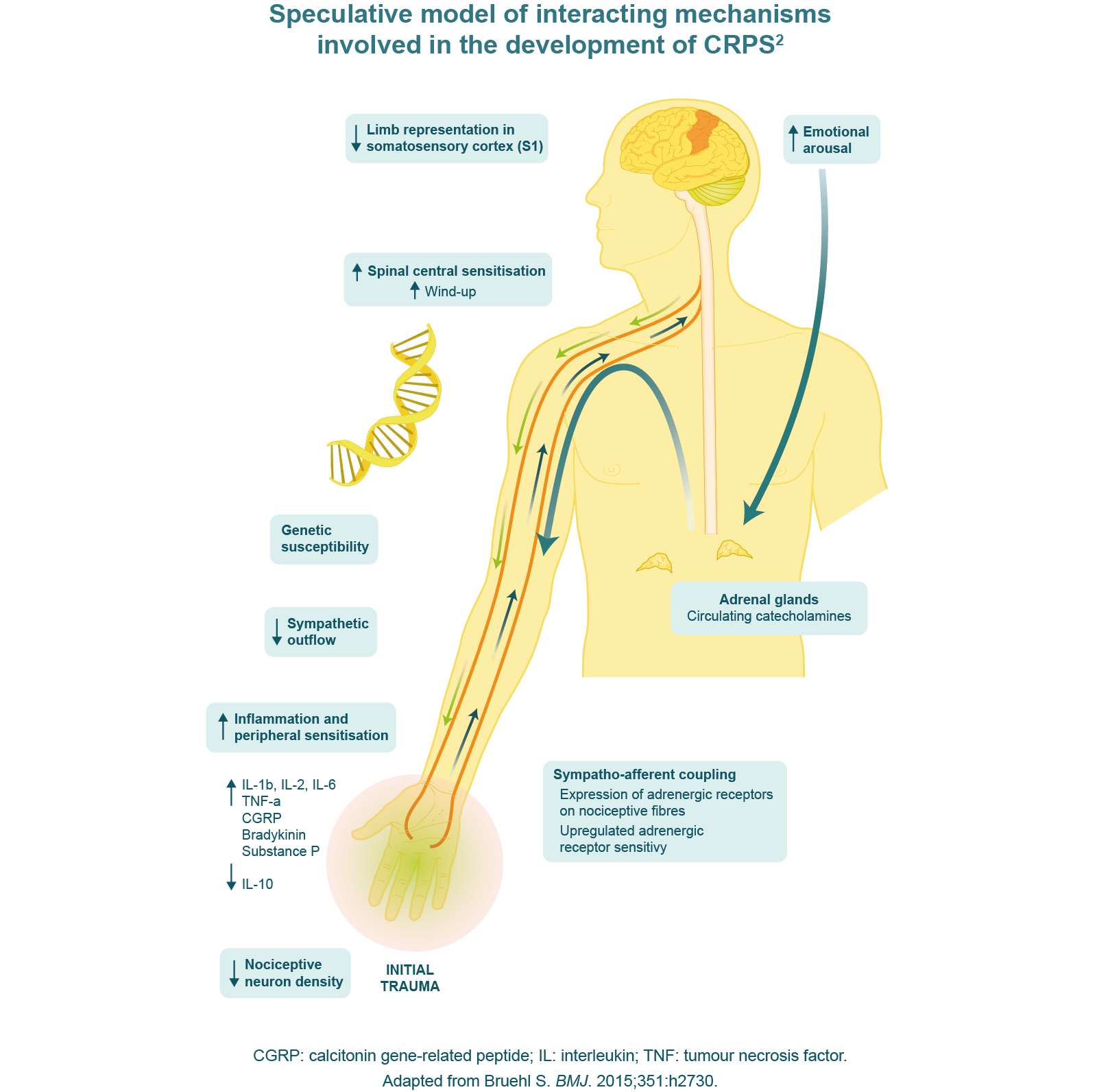
Following the initial trigger, CRPS is characterised by post-traumatic inflammation.6,12 Clinical observations are redness, swelling, hyperthermia, pain and reduced function of the affected limb.6,12 This is accompanied by a complicated immune response that involves proliferation of keratinocytes and production of inflammatory cytokines.6 In response to the original trauma, an exaggerated inflammatory response is triggered in CRPS;12 inflammatory mediators such as cytokines provoke pain and hyperalgesia through the sensitisation of peripheral nociceptors, which in turn facilitate the release of neuropeptides.6
Changes in the central nervous system can be responsible for the longevity of symptoms including allodynia, which is a result of central sensitisation.6 Symptoms can also be attributed to learned processes such as ‘learned non-use’ of the affected limb, as a result of initial pain caused by movement. Thereafter, an increase in pain occurs because of unphysiological movement to avoid pain.6 The peripheral nervous system has also been implicated in CRPS such that peripheral adrenoreceptors develop super-sensitivity and the sympathetic nervous system becomes more activated in the affected limb.6
CRPS can be subdivided into two types:1,3
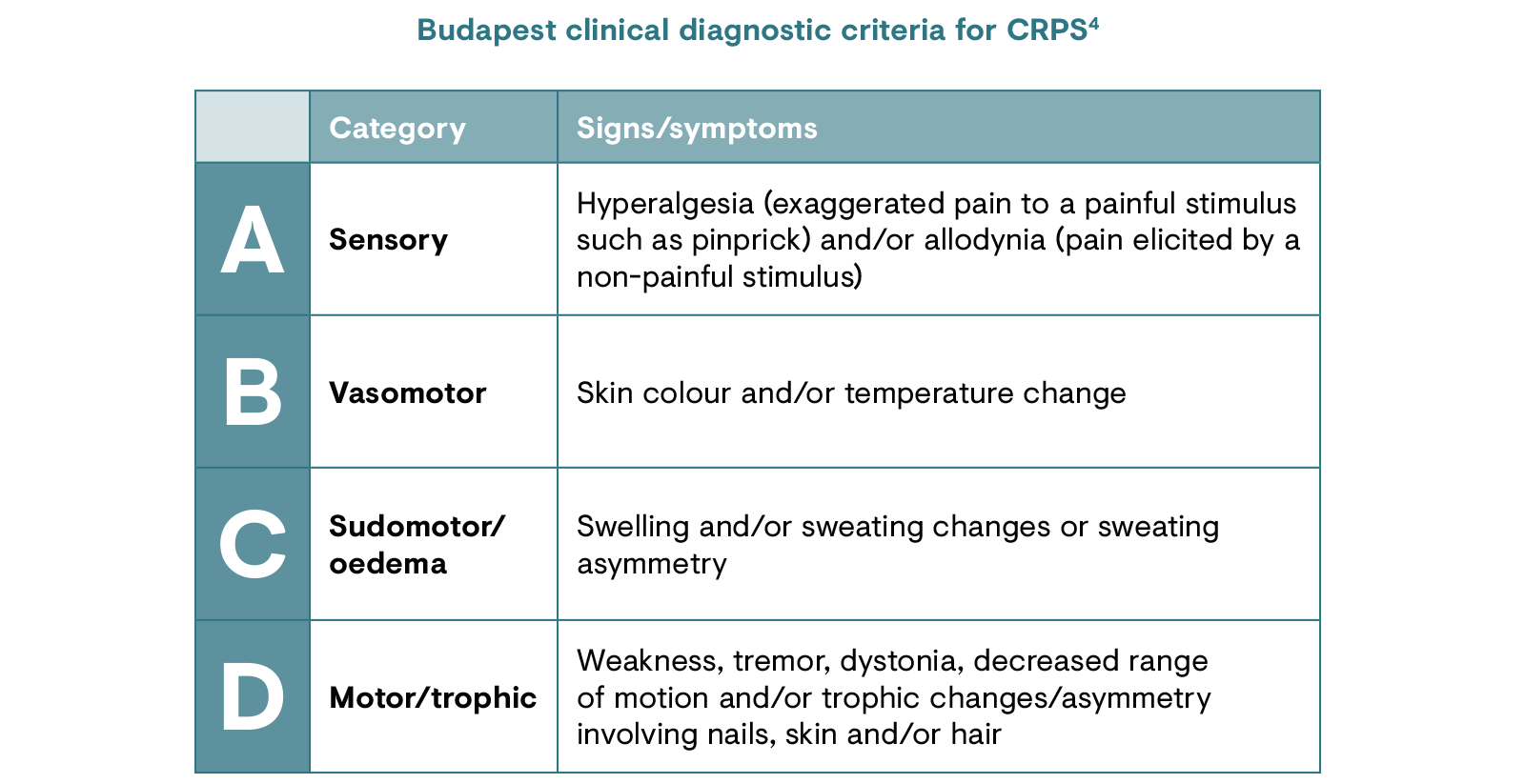
CRPS is diagnosed using the Budapest criteria such that:4
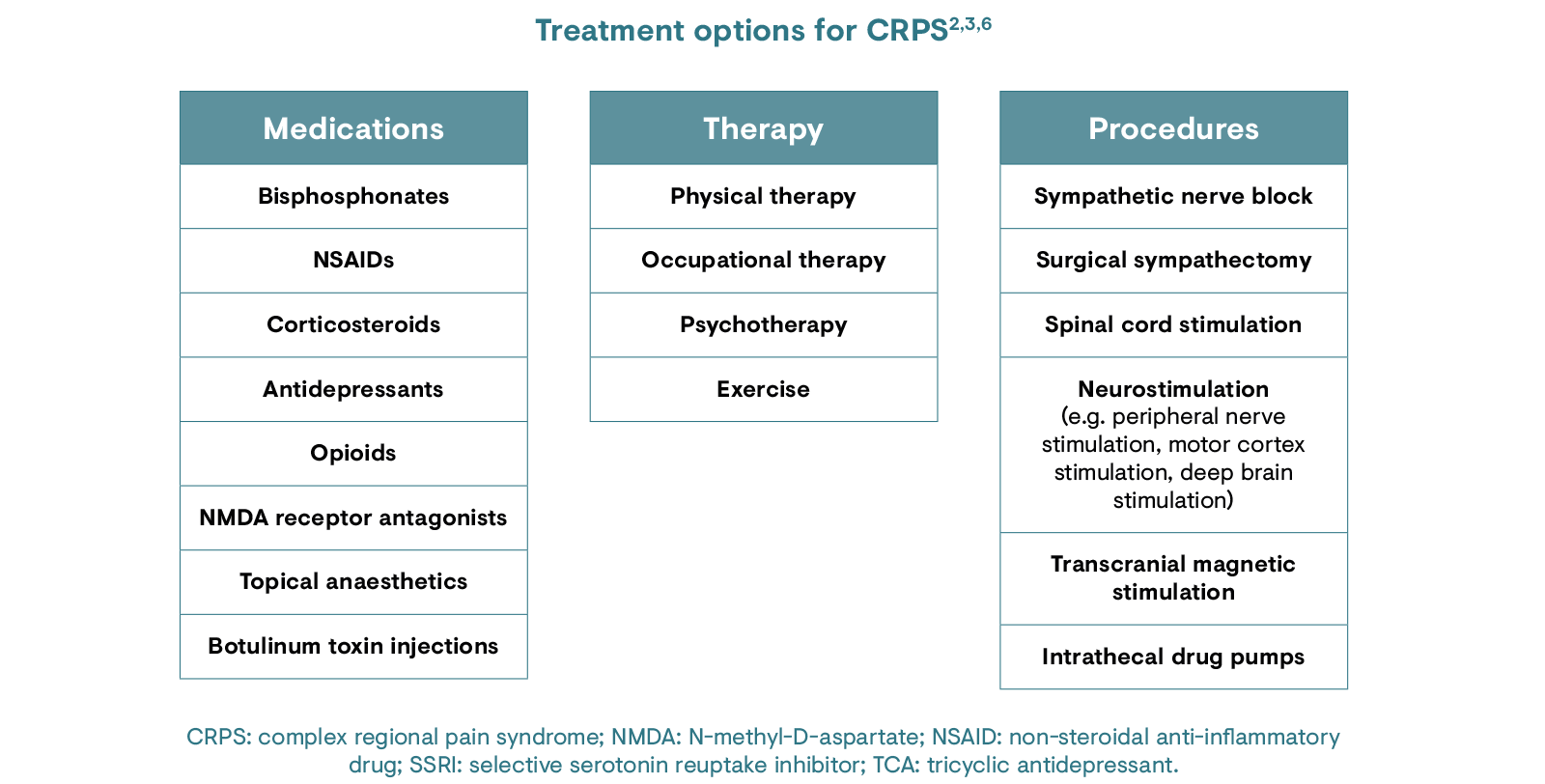
There is no cure or established standard of care for CRPS and it is a notoriously difficult-to-treat pain condition.3 General treatment guidelines have been published in the Netherlands13 and UK,14 but there is a lack of evidence-based treatment for CRPS management. The UK Royal College of Physicians presents the four pillars of treatment for CRPS: education, pain relief, physical intervention and psychological intervention. Although no drugs are licensed for the treatment of CRPS, there are several classes of medications that have been reported to be effective in CRPS.14 Surgical procedures have been utilised in some cases, but this approach remains controversial.3
Inadequate data are available to guide CRPS treatment solely on the basis of randomised clinical trial data, although trials suggest that the most commonly used intervention (sympathetic blocks) is probably ineffective for the average patient.2 An initial trial of oral corticosteroids is often used in patients with acute phase CRPS to dampen the large inflammatory component believed to be common in the acute phase.2
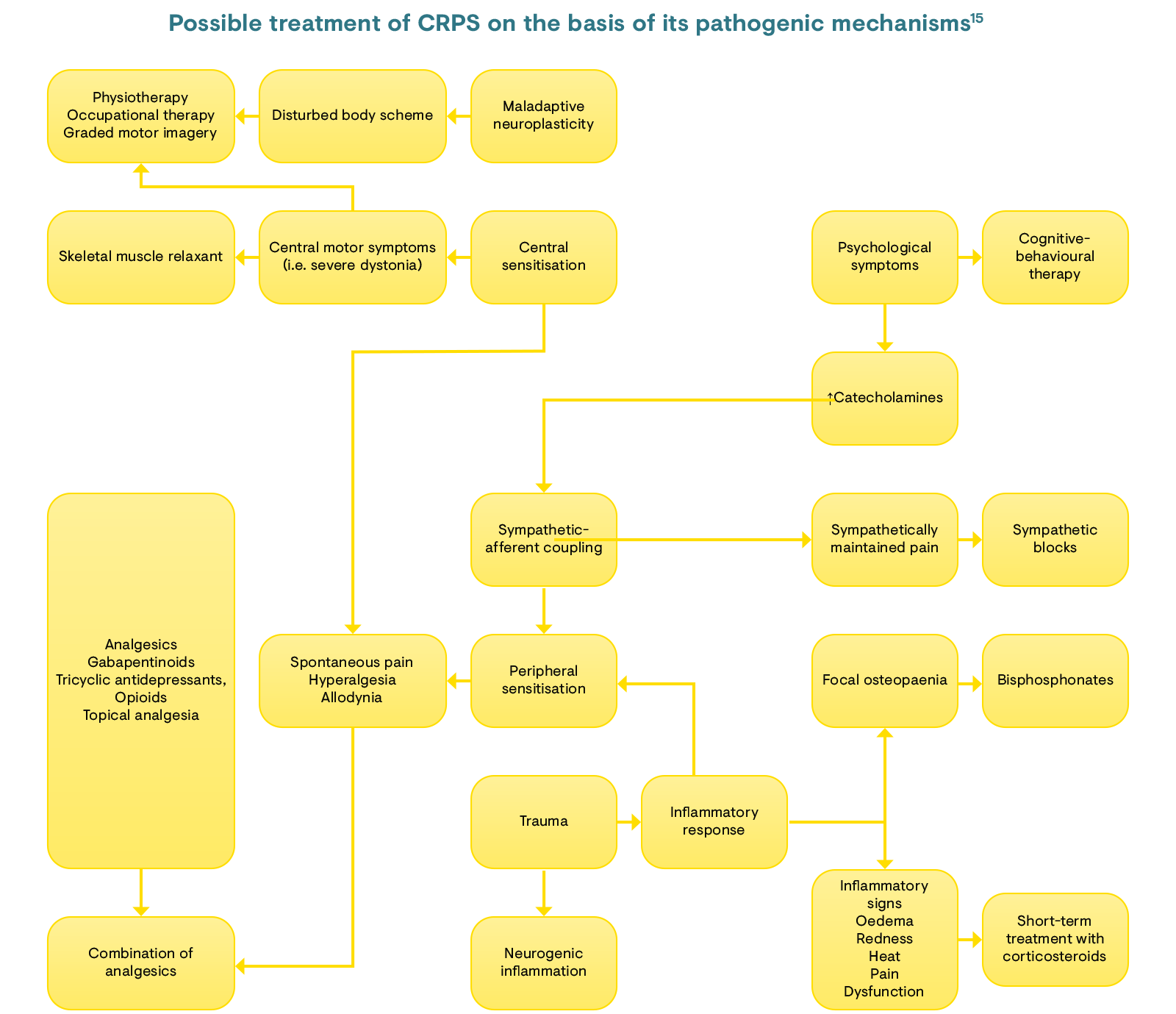
There are many different stages of the pain pathway that can impact CRPS, with trauma leading to inflammatory signs and dysfunction, and central sensitisation that can cause motor symptoms.15 Its management must therefore be multimodal to tackle the disease based on its pathogenic mechanisms and resulting symptoms.15 The algorithm below describes how the mechanisms of CRPS are interlinked and how the resultant treatment can be tailored on this basis.15 For example, physical therapy may be best suited for motor symptoms mediated predominantly by central sensitisation; corticosteroids or bisphosphonates for pain resulting from inflammation; and a combination of analgesics can be used to address spontaneous pain.15
A better understanding of the mechanisms underlying the pathophysiology of CRPS is needed. There is a lack of high-quality, multicentre, randomised controlled trials.6 Most of the available trial data are from single-centre investigations or lack a placebo arm.6 This may be a result of the low numbers of patients suffering from this disease. The National Institute of Neurological Disorders and Stroke, under the National Institutes of Health, is currently undertaking research into the various facets of CRPS pathophysiology – including immune system processes, inflammatory signalling pathways following cast immobilisation, and cellular and molecular changes in sensory neurons following peripheral nerve injury – to understand neuroplasticity and the role of neurotransmitters including adenosine triphosphate.3
Click here to register for CHANGE PAIN® and access in-depth educational resources on complex regional pain syndrome.
1. IASP. Classification of Chronic Pain, Second edition (revised). Available at: www.iasp-pain.org/files/Content/ContentFolders/Publications2/ClassificationofChronicPain/Part_II-A.pdf. Accessed April 2020.
2. Bruehl S. BMJ. 2015;351:h2730.
3. National Institute of Neurological Disorders and Stroke. Complex Regional Pain Syndrome Fact Sheet. 2019. Available at: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Complex-Regional-Pain-Syndrome-Fact-Sheet. Accessed April 2020.
4. Fukushima FB et al. BMJ. 2014;348:g3683.
5. De Mos M et al. Pain. 2007;129(1):12–20.
6. Birklein F & Dimova V. Pain Rep. 2017;2(6):e624.
7. Ott S & Mainhöfner C. J Pain. 2018;19(6):599–611.
8. Pons T et al. Anesthesiol Res Pract. 2015;2015:965639.
9. Elsharydah A et al. J Clin Anesth. 2017;39:34–7.
10. Roh YH et al. Arch Orthop Trauma Surg. 2014;134(12):1775–81.
11. Urits I et al. Curr Pain Headache Rep. 2018;22:10.
12. Perez RS et al. BMC Neurol. 2010;10:20.
13. Royal College of Physicians. CRPS guidelines. 2018. Available at: https://www.rcplondon.ac.uk/guidelines-policy/complex-regional-pain-syndrome-adults. Accessed April 2020.
14. Resmini G et al. Clinic Cas Min Bone Metabol. 2015;12(Suppl. 1):26–30.