PAIN BASICS
PATHOPHYSIOLOGY
Key points
- Pain can be described as being nociceptive, neuropathic and/or involving central sensitisation, which can lead to central plasticity changes.1
- Pain chronification describes the transition from the physiological response of acute pain to the more centrally sensitised condition of chronic pain, underpinned by changes in neuroplasticity.2
- Chronification is thought to involve biological factors, such as neuroplastic changes, and alterations in pain modulation and the way the brain processes pain.2
- It is imperative for healthcare professionals to understand the mechanisms that underlie common conditions in which chronic pain arises so that they can make an informed decision about management options for their patients.2,3
Pain mechanisms
The development and persistence of pain is typically attributed to three mechanisms of pain pathophysiology – nociceptive, neuropathic and central sensitisation – that may act independently or in combination (Figure 1).1,2
Nociceptive pain
Nociceptive pain typically originates from tissue damage caused by trauma, non-healing injury or inflammatory processes, and can be divided into two categories: somatic pain (injuries of the musculoskeletal system) and visceral pain (internal organ injury, often felt indirectly).1,4,5 In response to actual or potentially harmful chemical, mechanical or thermal stimuli, the two types of primary afferent nociceptors, Aδ- and C-fibres, transmit nerve signals to the dorsal horn of the spinal cord and ascending cortical pathways to the brain.1 If the pain threshold for normal tissue damage is exceeded, peripheral sensitivity to subsequent stimuli increases.1 While sensitisation is only temporary if subsequent stimuli are short in duration, the continuous presence of stimuli and resulting sensitisation may lead to changes to the peripheral nerves and central nervous system.1
Neuropathic pain
Neuropathic pain is classically caused by lesions within, or diseases that affect, the somatosensory nervous system.1 Another cause of neuropathic pain is injury or trauma during surgery.1 Following nerve injury or damage, disordered neural processing in the peripheral or central nervous system, as well as cell death, may occur.1 Such changes can lead to abnormal pain sensations.1
Central sensitisation
Central sensitisation (also known as nociplastic pain, sensory hypersensitivity or central hypersensitivity) manifests as the perception of pain in the absence of pain receptor activation.1,4 As a result of the neural remodelling that underlies central sensitisation, sensitivity of afferent nerve fibres is increased such that a stimulus that would be deemed non-harmful under normal conditions now triggers a pain response.2 This phenomenon is driven by hundreds of molecular changes.1
Figure 1: Three types of pain pathophysiology underlie chronic pain conditions.
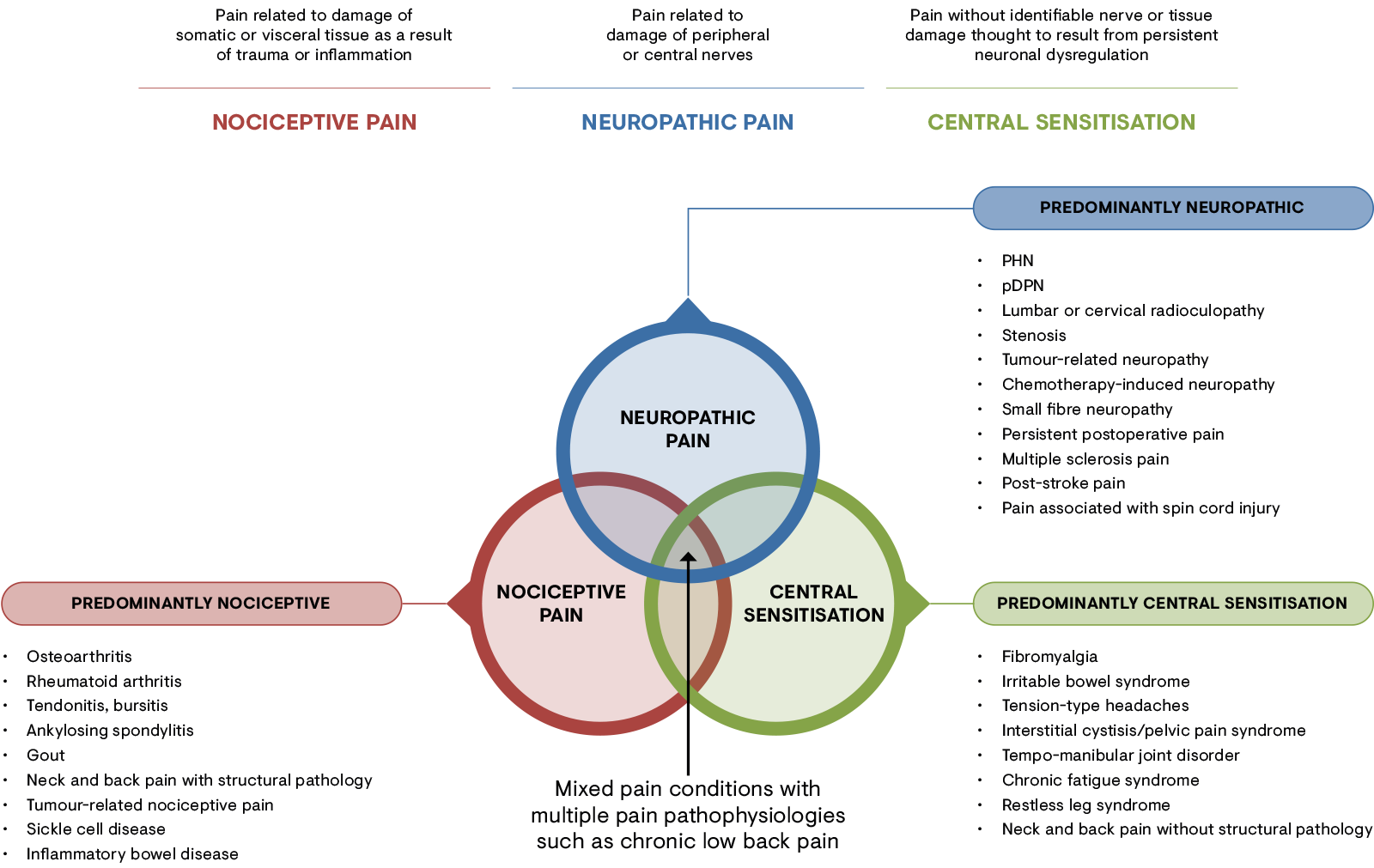
(A) The three main types of pain pathophysiology give rise to chronic pain conditions. (B) These types of pain may present separately or in combination to contribute to the overall pain experience.
pDPN: painful diabetic peripheral neuropathy; PHN: post-herpetic neuralgia.
[Adapted from Stanos et al. 2016.4]
Pain chronification
The chronification of pain, whereby changes in neuroplasticity underlie the transition from acute to chronic pain, is an area that is not fully understood.2 Chronic pain may involve possibly irreversible pathophysiological changes; therefore, understanding and interrupting the cascade of events that occur during the development of chronic pain is key in its effective management.2
It is clear from recent pain models that multiple interacting factors that extend beyond the initial triggers of pain contribute to the development and maintenance of chronic pain.1 Contributing biological factors include neuroplastic changes, altered pain modulation and changes to the way the brain processes pain (also called the neuromatrix).2 Changes in the neuromatrix are characterised by increased brain activity in areas that process acute pain, alongside brain activity in areas not known to be associated with acute pain signal processing.2 Psychological risk factors are another important consideration; negative affective constructs such as anxiety, depression, pain catastrophisation and general psychological distress have been consistently identified as risk factors in some chronic pain conditions such as chronic post-surgical pain.6
-
References
1. Clauw DJ, Essex MN, Pitman V, Jones KD. Reframing chronic pain as a disease, not a symptom: Rationale and implications for pain management. Postgrad Med 2019; 131: 185–98.
2. Pergolizzi JV Jr, et al. Pain Manag Nurs. 2014;15(1):380–90.
3. Godfrey H. Br J Nurs. 2005;14(16):846-52.
4. Stanos S et al. Postgrad Med. 2016;128(5):502–15.
5. Orr PM et al. Crit Care Nurs Clin N Am. 2017;29:407–18.
6. Weinrib AZ et al. Br J Pain. 2017;11(4):169–77.